
原文刊载信息:
IEEE Trans Radiat Plasma Med Sci. (《IEEE辐射等离子医学科学杂志》)2020 Jul; 4(4): 391–399.
Published online 2020 Jun 16. doi: 10.1109/TRPMS.2020.3002658
PMCID: PMC8043491
PMID: 34192214
原文标题:Gas Plasma Technology—An Asset to Healthcare During Viral Pandemics Such as the COVID-19 Crisis?
作者信息:Sander Bekeschus,corresponding author1,2 Axel Kramer,3 Elisabetta Suffredini,4 Thomas von Woedtke,1,5 and Vittorio Colombo6
COVID-19危机深刻揭示了人类社会和医疗保健系统在大流行情况下的脆弱性。在许多情况下,迅速安全地减少病毒载量和传播是成功管理此类大流行的首要原则。然而,人们也看到了医疗保健领域的许多既定程序并不总是足以应对对物品、医疗产品甚至受感染组织的去污染需求不断增加的情况。在过去25年中,气体等离子技术的使用在其除菌性能方面引起了大量的文献关注,特别是对于热敏目标,如聚合物和组织,化学去污染通常不适用。然而,虽然早期研究的重点大多集中在细菌上,但关于病毒灭活的报告相对较少。我们旨在向广大受众展示在COVID-19这类的病毒大流行期间气体等离子技术在医疗卫生领域的机会与潜力。这包括可能的现实世界气体等离子应用、适当的实验室病毒测试系统以及有关气体等离子体进行病毒灭活的技术和安全要求的关键点。
关键词:
空气传播病毒、常压低温等离子体、DBD、消毒、等离子喷射、传染。


迄今为止,在21世纪全球范围内对人类社会、金融和医疗保健系统影响最大的事件是“COVID-19大流行”。尤其令人恐惧的是,由于“严重急性呼吸综合征冠状病毒2”(SARS-CoV-2)病毒在感染人群说话、呼吸和咳嗽时释放的气溶胶飞沫中传播,其全球扩散速度非常快。这场大流行毫不留情地摧毁了医院、疾病诊断和公共生活在处理极具传染性病原体方面的缺陷。与此同时,许多政府也展示了前所未有的灵活性和愿意应对每天不断变化的状况的意愿。可以希望,全球社区在2020年意识到,需要建立一套强有力的保护策略来应对像这样的卫生危机,因为在其他疫情爆发时,这种策略也将绝对需要,它的致死性可能超过当前COVID-19的情况,20世纪初的西班牙流感证明了这一点。
抗击疫情的关键是打破感染链。这意味着不仅通过限制性措施避免感染者传播病毒,还要通过在受污染的物品和设备上实施严格的消毒措施,对室内空气进行脱除污染物的处理,特别是在混合通风的手术室以及其他需抗菌的环境中,关于预防和治疗方面也需要进行一定的处理。虽然大部分酒精等传统消毒方式适用于大多数应用场景,但某些情况下通过优化的消毒程序确实也有助于限制病毒的传播。在过去的几个月中,通过与各学科领域内和跨学科同事以及社会利益相关者讨论气体等离子技术在减少病毒负载方面的优势,我们得出结论,其他等离子体消毒技术在某些方面可能比现有的方法更有优势。在简要介绍后,我们概述了在COVID-19这样的疫情期间气体等离子技术有何等价值。我们的目标是以一种可理解于物理学家、生物学家、社会利益相关者、医学博士和医疗保健从业者等许多学科的科学家为参考的方式提供信息。毕竟,历史已经表明,将来自不同领域的想法汇集起来往往是寻找新解决方案的关键,例如需要替代或补充病毒灭活方法以升级现有程序,这是最近COVID-19病毒大流行所教给我们的悲惨教训。
A. 病毒劫持
作为被称为新型冠状病毒病(COVID-19)的大流行病的病原体,“严重急性呼吸综合征冠状病毒2(SARS-CoV-2)”是一种与呼吸系统和其他器官和系统感染有关的病毒。与真核细胞(如人体细胞)和原核细胞(如细菌)不同,病毒没有自维持的新陈代谢。这基本上意味着,真核细胞和原核细胞可以依据环境中的营养物质生存和繁殖,而病毒无法自我复制。相反,它们需要一个宿主细胞来执行病毒复制工作。病毒通过劫持宿主细胞生产必要的蛋白质和核酸来构建新的病毒颗粒。对于某些类型的病毒,这也可能涉及脂质。最终,感染病毒的细胞变成了病毒生产工厂。在连锁反应中,新的病毒颗粒可以进入相邻的细胞并感染它们,或者它们可以利用现有的出口途径(即呼吸系统或消化/泌尿道)被运送到体外。
B. 病毒突变
从生物学的角度来看,承认地球上所有的生物体都与病毒共同演化是至关重要的。病毒感染已知在细菌(例如噬菌体攻击细菌)、真菌、植物和脊椎动物中出现。据推测,人类和许多其他生物的DNA包含许多最初来自古代病毒基因组的区域,这显示了生命细胞与“寄生”DNA的长期互动。病毒的另一个重要方面是,它们在核酸序列方面比真核生物进化得更快。在宿主细胞中的复制中,病毒核酸序列复制会积累错误。其中一些复制错误对病毒有利(例如通过增加其感染或潜伏率),一些没有效果(中立),最后,还一些复制错误还会对病毒传播产生有害的影响。
2003年的SARS冠状病毒,首次通过航空旅行传播[2],显示出其具有一定的突变率[3],报道称SARS-CoV-2的进化速率也与之类似[4]。目前,核酸序列的改变被用于跟踪2020年全球COVID-19大流行的传播路径。现今,测序技术快速、准确且廉价,因此这些突变可以用于分离当前大流行病冠状病毒的不同变异体[5]。毕竟,了解到从病毒的角度来看,以适度致死率换取最大扩散是可取的,因为迅速杀死宿主最终会也会杀死病毒,反而打断病毒传播的机会。
C. 冠状病毒是包膜RNA病毒
病毒可以根据多个标准进行分类,其中之一是是否有包膜。另一个标准是病毒复制所需信息存储在DNA还是RNA中。与流感病毒类似,冠状病毒是一种包膜RNA病毒。包膜实际上是宿主细胞膜上镶嵌着病毒蛋白的一部分,是决定消毒灭病毒效果的因素之一[6],[7]。DNA和RNA病毒在许多方面存在差异。DNA病毒的基因组通常更稳定,比RNA病毒大,且复制准确。相反,RNA病毒的基因组不太稳定,在复制过程中容易出现错误(由于病毒基因组内编码的RNA聚合酶缺少校对活性),且通常编码的长度更短(基因组更小)。一些DNA和RNA病毒可以整合到宿主细胞的基因组中处于“休眠”状态,等待细胞压力和病毒复制等条件的触发。其中一些众所周知的病毒包括单纯疱疹病毒、人免疫缺陷病毒和乳头状瘤病毒。这些病毒可能会在宿主体内永久存在。相反,一些最具流行病学意义的RNA病毒(例如,导致胃肠炎病毒的大部分病毒以及肠道病毒,如脊髓灰质炎病毒、乙肝病毒方程式M1和方程式M2等)在宿主细胞质中复制并迅速散布至高浓度的病毒颗粒到环境中,只很少出现长期存在于宿主体内的情况。常见的RNA病毒包括诺如病毒、埃博拉病毒、麻疹病毒和冠状病毒。因此,在评估灭菌研究文献时,病毒多样性的这些方面非常重要。与细菌类似,研究不同物种的差异越大,从一个物种到另一个物种的任何结果转化都越差。如果读者对病毒分类和形态内病毒分歧感兴趣,可以查看2020年5月发布的最新病毒15级分类层次结构[8]。
A. 气体等离子技术原理
物理等离子体是一种激发态气体,有时也被称为“第四状态”,可以通过不断向中性气体的原子或分子供能来产生。即使所需的能量可以通过热、化学、电和辐射资源分别或通过所有这些资源的组合单独提供,但主要的电离机制是涉及非弹性碰撞、电子撞击、辐射相互作用和电荷交换的碰撞过程。激发态的典型寿命约为10纳秒,即如果能量供应停止,将开始耗尽过程,迅速熄灭等离子体。生物医学等离子体最有效的产生方法是基于强电场的电子撞击电离。电子能量通过与气体中的原子或分子的非弹性和弹性碰撞转移,导致其完全或部分离子化。部分离子化气体的温度始终远低于特征电离温度。根据等离子体源的设计,可以实现等离子体环境的常温,使其非常适合治疗热敏表面和材料。复杂的物理化学等离子特性取决于许多参数,包括用于等离子产生的气体或气体混合物的类型和组成、应用的能量和电极配置、压力和环境。关于其应用,特别是在医疗领域,有用的分类是热等离子体与非热等离子体,以及低压力与大气压等离子体[9]-[11]。
在等离子医学作为一个新的领域不断发展的最近几年中,德国已经对四种冷等离子源进行了医学临床试验,并获得了医疗设备许可。它们可以直接作为介质屏障放电(DBD)或间接表面DBD或等离子喷嘴运行[12]-[14]。这些来源的好处是它们可以在大气压下在环境(“室内”)空气中运行,具有与人体温度类似的温度,稳定且易于操作,在制造方面相对成本效益。
B. SARS-CoV-2在各种环境中的存活情况
SARS-CoV-2病毒主要,通过插管、支气管镜、鼻镜或外科手术干预作为气溶胶从呼吸道释放出来[15]和[16]。 SARS-CoV-2在血液中也可以检测到,患病率为15%,可能在手术干预期间污染手术团队[17]。该病毒也存在于25%-80%的大便样本中,可能导致医院和家庭环境和表面污染,并需要准确的表面消毒[18],[19]。 SARS-CoV-2可以在室内空气中作为气溶胶存活3小时。在铜表面经过4小时和纸板经过24小时后,可以检测到无感染性病毒颗粒[20]。在两天和三天后,可以在不锈钢和塑料载体上仍然检测到活病毒。在更高病毒滴度的SARS-CoV-1的类似研究中,病毒保持完好达6天[21]。因此,需要针对室内空气和表面杀灭SARS-CoV-2等呼吸道病毒的方法。
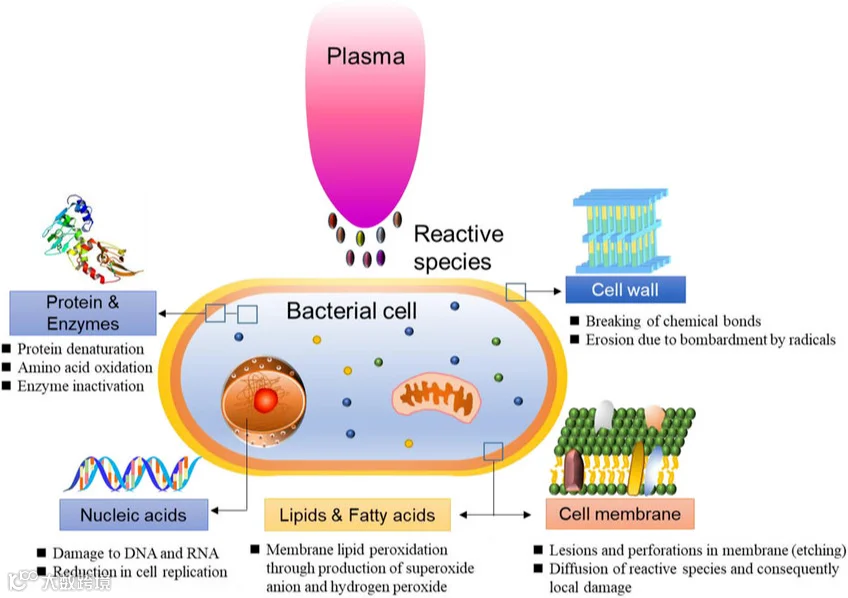
当需要抗菌、抗病毒和/或抗生物膜活性时,气体等离子技术的使用在卫生指示方面是成功的或有前途的。这尤其适用于对化学微生物灭活剂具有热敏性或敏感,并且当微生物杀灭剂无法或只能不足地到达作用点时。由于气体等离子体具有高度有效的抗菌成分,其活性谱包括所有营养菌物种,包括多重耐药菌,广泛的病毒[22],甚至以极高耐受性而闻名的朊病毒。由于其作用方式,尚未观察到气体等离子处理的内在耐药性[23]。使用气体等离子体进行表面上消毒时能够在2分钟内灭活呼吸道病毒,如禽流感病毒和新城疫病毒[24],以及在5分钟内灭活人类呼吸道合胞病毒(RSV)[25]。一个未解决的问题是在手术室中通过混合通风对室内空气进行消毒,特别是在骨科和创伤干预期间,因为来自呼吸道和血液尘埃的混合传染性气溶胶会危及手术组。通风系统可能会增加手术团队对SARS-CoV-2的暴露。仅当具有直接将排气从手术室排出到外部的层流气流,并且如果能将通风系统切换到负压,那么感染的风险才是最小的。对于在COVID-19患者上进行骨科和创伤手术的手术室,通常使用具有湍流机械通风或没有通风的设备都是不可取的方案。目前一个安全的技术解决方案是利用一种创新的移动过滤系统,首先通过一个M5预过滤器吸入室内空气。然后,空气通过G4碳褶皱滤器,并通过使用气体等离子体场将吸入的空气从微生物中去除,包括病毒,并在同时进行解毒(例如过敏原和异味污染)。然后将纯净的空气通过HEPA 13过滤器反馈到室内,该过滤器完全保留微生物,然后通过单位的顶部经过G4褶皱碳过滤器(目前正在进行NCT02695368的临床试验)。在使用MS2噬菌体作为流感病毒的代用品进行的概念证明研究中,在室内空气中通过雾化后15分钟内已灭活99.99%(4对数)的病毒颗粒(来自气溶胶研究和工程实验室的Balarashti和Conley的未发表观察) 气体等离子体对MS2噬菌体的活性的想法在其他两项研究中得到了强调,在这些研究中仅在0.12秒[28]和0.25秒[29]的接触时间内使用气体等离子技术就成功灭活了气溶胶。
C. 气体等离子体作为灭菌的通用工具
将气体等离子体应用于灭活、杀死或清除病原体的研究已经超过50年。最初,对于材料和设备的抗菌处理,都是利用常压等离子体上完成的。1990年代中期开始的常压等离子体设备的普及,加强了其用于抗菌处理的研究。尽管在许多情况下都使用了术语“等离子灭菌”,但尚未开发出满足灭绝基本消毒要求的真正基于等离子体的灭菌过程或设备[30]。尽管由于多种实际和监管原因,气体等离子处理可能不适合取代或完全补充经典的灭菌处理,但在卫生和医学的特定消毒场合,传统的基于热、辐射或有毒化学物质的方法无效或不适用时,运用气体等离子处理有着巨大的潜力。[31]-[38]。
大规模的等离子体设备具有巨大的经济和医疗潜力。 COVID-19疫情导致医院消毒能力严重不足。使用气体等离子技术的等离子体支持的过氧化氢气体灭菌已经是常规和/或传统灭菌方法的有效替代品,也是消毒高分子材料和热敏性医疗设备的不可或缺的创新[39] - [41]。在食品加工方面,广泛的研究活动已经带来了一些非常高的技术转移水平(TRL)[42]。这涉及处理食品,研究等离子处理对不同基质中的食品成分和质量的影响,以及在食品安全和包装技术方面增加产品的保质期等方面。在水处理领域,与液体接触的非热等离子体作为高效氧化降解手段的能力也得到了研究,因为传统处理无法去除不可生物降解的药物化合物[38],[43]。
另一个充满挑战但很有前途的应用是使用气体等离子技术进行消毒。已经证明,气体等离子在皮肤[44] - [46] 和伤口[47]的使用上具有很好的耐受性,并且类比于粘膜组织的应用也是可行的。由于(指发文时)COVID-19 的疫苗尚未推出,为了特别保护医护人员,必须竭尽一切可能的卫生预防措施。在最大程度保证功效和安全的情况下,使用等离子体设备可以作为酒精手消毒的补充或替代。气体等离子可以高效消灭健康志愿者指尖上的生理性和非生理性微生物[48],气体等离子治疗也具有很好地耐受性,既不损伤皮肤屏障,也不引起皮肤干燥[49]。然而,为了使气体等离子手消毒变得实用,需要通过技术手段大大减少等离子体暴露时间。
D. 气体等离子处理病毒
针对使用气体等离子技术在减少和控制病毒通过飞沫传播、降低疾病负担和控制医院内呼吸道病毒的院内感染方面的应用,Terrier等人的工作[50]应得到重视。通过常温氧等离子体和紫外线的结合,高浓度悬浮的流感病毒M3型、人类副流感病毒3型和RSV病毒得到处理。该系统是由一个单通道流通隧道组成,其中微米级被污染的飞沫经过雾化处理,然后在内部气体设备(与紫外线混合的等离子)中进行处理,同时在设备反应前后对空气进行取样。对该系统的运行条件进行了病毒灭活效果测试,报告了高达6.8个对数的降低。对于液体中腺病毒的灭活,Zimmermann等人[51]使用了在空气中运行的平面表面介质屏障微放电技术。同样观察到很强的病毒灭活效果,在4分钟的气体等离子暴露后,灭活效果高达6个对数。Brun等人[52]对单纯疱疹病毒1(HSV-1)16型进行了研究,他们使用的是基于氦流离子化的等离子源。然而,在等离子处理后未观察到病毒的感染性降低。另一项研究在体外对人角膜上皮细胞和植入角膜中的HSV-1进行了气体等离子处理,但未发现明显的毒性。同时观察到了明显的抗病毒活性。结果表明,在对抗耐药单纯疱疹角膜炎时,将气体等离子转化为临床治疗的良好机会[53]。另一种持续困扰患者和医疗领域的病毒是肝炎病毒B(HBV),特别是在为患者生成供血的输血医学中。利用直接DBD,含HBV抗原的血液接受气体等离子暴露。等离子处理降低了粒子的抗原性,同时显著干扰红细胞的稳态并引起溶血。可以得出结论,至少在给定的设置和全血状况下,气体等离子不适用于使血液样品免于病毒污染[54]。HIV也是输血医学的一个问题。Volotskova等人使用一种不同于血液的模型,研究了用氦等离子喷射器处理对单核细胞衍生的巨噬细胞(MDMs)HIV-1复制的影响。观察到了等离子处理的抗HIV活性,对病毒-细胞融合、病毒逆转录和整合以及气体等离子处理的细胞产生的病毒颗粒表现出减少的感染力[55]。在另一项有关HIV的研究中[56],Amiran等人使用氦喷射器的等离子体暴露HIV。结果显示,在电压和等离子处理时间增加的情况下,HIV的抑制增强,但已经对作为感染模型的HeLa细胞具有毒性,因此不鼓励在特定的模型中采用这种方法。以上所有研究都是在大气压下进行的。在非大气压下,氮气等离子体对流感病毒及其组分的病毒杀灭作用也被观察到[57]。
通过使用噬菌体可以轻松测试抗病毒活性。在挑战之后,可以通过噬菌体溶解细菌的效力来评估其感染能力。Wu Yuqing等人研究了防止病毒媒介通过空气(和水)传播的新策略。他们使用DBD等离子源置于暴露室中,并注入MS2悬浮液的气溶胶病毒,研究了等离子辅助下对MS2噬菌体的灭活[28]。为了测试水生条件,对同样的MS2噬菌体进行了处理,但它处于悬浮状态而非气溶胶状态。对于空气和水生状态下的MS2病毒的灭活,这取决于功率、暴露时间和载体气体,主要归因于等离子生成的活性氧物质,其介导了对病毒表面蛋白和RNA的氧化损伤。同样地,Guo等人研究了通过DBD表面等离子体系统产生的氧和氮活性物质对含有替代病毒噬菌体中水分子的病毒灭活机制。等离子体处理有效地损伤了噬菌体的蛋白质和RNA。此外,与直接等离子处理相比,处理过的等离子体水同样有效,这表明长寿命的活性物质 - 可以通过化学手段轻松制备 - 成为介导灭活的主要因素[58]。噬菌体还被用作一个模型,以展示旨在防止空气传染疾病传播的工业规模原型的抗病毒活性[29]。在气流中的病毒气溶胶(高达330 L/min)在填充床反应器中接受了非热等离子体处理,其中发现DBD处理会随着施加电压的增加去灭活气溶胶的MS2噬菌体。还特别注意对残留臭氧的下游处理,使用活性炭过滤器进行处理。总的来说,最近有一份更全面地对气体等离子体研究中病毒灭活的综述已经发表[59]。
虽然这些研究大多数在机制和氧化还原化学方面描述得相当详细,但Bruggeman小组发表了一项复杂的研究,对这些方面进行了更深入的探讨。他们使用了一台远程射频等离子体源、猫病毒性口炎病毒、一系列供料气体组成以及数十种不同的自由基清除剂[60]。简而言之,他们发现了两种等离子体诱导的化学反应,每种具有独特的灭活途径,其中一种是基于单线态氧,另一种是基于过氧亚硝酸。总的来说,必须承认,气体等离子体辅助病毒灭活的机理并不完全清楚。可以假设病毒颗粒经过破坏性氧化和解体,进而失去了感染能力。与真核细胞不同的是[61]-[65],不能排除等离子体源产生的ROS和RNS直接对病毒DNA造成损伤的机制,因为病毒中缺乏保护的细胞质和多种细胞膜。显然,在等离子体处理的真核细胞[66]-[69]中观察到的编程细胞死亡程序和氧化还原信号事件也不会在病毒中被触发。
A. 用于冠状病毒研究的实验室测定
评估气体等离子技术用于灭活经气溶胶传播的病毒(如冠状病毒CoV)的功效,依赖于使用实验室测定检测病毒的感染力。病毒感染宿主是一个复杂的过程,涉及几个步骤(如附着、穿透、脱壳、复制、组装和释放新的病毒颗粒),每个步骤都需要特定病毒结构和整个病毒的功能完整性。其中,附着蛋白的功能性、病毒外壳的完整性以及病毒基因组的完好无损都是实现感染宿主细胞的必要条件。由于所有这些病毒结构可能单独或同时受到气体等离子体处理的影响,因此需要复杂的体外系统,如允许重现感染周期所有阶段的永生细胞系,来评估病毒感染力。这种需求本身就对测试有所限制,因为细胞培养系统需要专用实验室环境和高度训练的人员来进行有效实施。
此外,在与气体等离子技术相关的病毒测试中,还应全面考虑以下几个问题:
1)
细胞培养系统的可用性:虽然多种临床感兴趣的病毒可以在细胞系中轻松培养,但是像诺如病毒和小冠状病毒这些高度相关的人类病毒病原体尚未有效培养出来。
2)
感兴趣的病毒的生物安全等级(BSLs):包含高致病性呼吸道冠状病毒(如SARS、MERS和SARS-CoV-2)的诊断标本可以在BSL-2实验室中进行处理,并配备额外的人员防护设备(包括但不限于一次性手套、袖口带袖口的防护服、眼睛保护、全面防护面罩、强化消毒程序等)。然而,为了在细胞培养中繁殖这些病毒(如Vero E6细胞),严格要求BSL-3设施和工作实践(请参见2003年4月25日的世界卫生组织SARS标本处理生物安全指南、中东呼吸综合征冠状病毒相关标本处理的临时实验室生物安全指南(版本2)以及有关新冠病毒的实验室生物安全指南的临时指南,时间为2020年2月12日)。
由于缺乏体外培养系统或由于生物安全的限制,往往需要在实验环境中使用替代病毒,即通常预期可以模仿所代表病毒行为而不会造成同样的技术和分析问题的病毒。就冠状病毒而言,由于结构和基因的相似性(外壳大小、存在包膜和ssRNA基因组),通常会导致轻度到中度呼吸道疾病(如普通感冒)的人类致病性冠状病毒可以作为高致病性冠状病毒的代用品。这些病毒包括alpha-CoV类型的229E和NL63以及beta-CoV类型的OC43和HKU1,分别可以使用MRC-5,LLC-MK2,HCT-8和HAE细胞培养在BSL-2环境中培养[70], [71]。然而,应考虑到,尽管这些菌株的病原性较低,但在选择任何实验计划之前,应评估与实验室人员暴露于这些呼吸道病毒的潜在风险。
在考虑到这些限制的情况下,动物冠状病毒经常被提出作为SARS和MERS的代用品。例如,猪和猫的alpha-CoV可以通过可传染性胃肠炎病毒(TGEV)和猫传染性腹膜炎病毒(FIPV)等病毒作为代用品,重复使用来评估从水矩阵和空调/通风系统中回收CoV的效果[72], [73],不同化学处理的病毒灭活效果[74], [75]以及水或表面上的CoV存活[76]- [78]。同样,像牛冠状病毒和小鼠肝炎病毒(MHV)等beta-CoV已被用于杀菌剂的研究[75], [79],分析方法的验证[80], [81]以及持久性研究[76], [77]。最近为克服生物安全问题,提出了使用CoV假病毒颗粒(即,在不同的病毒骨架结构上组装相关病毒特征而获得的不完整病毒)来研究SARS-CoV-2感染机制[82],[83],这一发现为在其他需要使用代用品的领域中也可能应用融合病毒提供了可能性。
虽然使用人/动物冠状病毒代用品确保了病毒结构的高度相似性,从而支持将结果推断到感兴趣的病毒,但代用病毒的代表性概念已受到质疑[84]并指出,负责动物肠道或肝病的代用冠状病毒可能在环境和治疗中表现出不同的耐药行为,与人类呼吸道冠状病毒[85]不同。除此之外,使用人/动物冠状病毒代用品并不能克服与细胞培养系统复杂性相关的大多数可行性问题。实际上,除了需要专门的环境和专业人员外,细胞培养系统还极大地受到与实验设计以及特别是用于测试的基质相关的问题的影响。虽然病毒悬浮液矩阵受到气体等离子体处理后可以轻松进行直接细胞培养测试,但固体表面(无论是惰性还是有机的,在食品等离子体研究中的情况更是如此)上的病毒回收却带来了几个问题,包括如何:1)实现适当的回收效率以保证结果的可靠性;2)尽量减小对病毒结构的损害,避免在待测处理下进行不正确的失活评估;和3)实现适当地去除所有基质残留物,以减少对细胞系的干扰和毒性影响。
为了避免这些问题并减少对细胞培养的病毒测试的技术复杂性,通常会提出替代策略,主要是通过使用细菌病毒(噬菌体)来实现。噬菌体的检测/枚举应用传统的细菌学技术,并且受到测试部分中基质残留物的影响较小。因此,不同的噬菌体已被用作CoV或更一般地用于包膜病毒的代用品,其中包括Enterobacteria噬菌体MS2(Leviviridae家族)或Pseudomonas phi噬菌体(例如M5方程式或M6方程式,Cystoviridae家族)[80],[86],[87]。然而需要注意的是,噬菌体行为的代表性似乎对气溶胶传播的病毒具有变化性[88],而且这些代用品都不能与CoV完全对应(非包膜病毒的MS2噬菌体和具有分段双链RNA的phi噬菌体) 。规避细胞培养病毒的其他方法包括使用“活力PCR”,即专门设计的分子分析方法,以评估病毒外壳或基因组(或更少见的两者)的完整性。这些方法依赖于特定的分析策略,如使用长模板PCR,覆盖大片段或理想情况下整个病毒基因组来评估其完整性,或使用核酸插入剂,如乙啶单偶氮苯或丙啶单偶氮苯(EMA或PMA),以阻止PCR扩增其中失去外壳完整性导致病毒RNA暴露的病毒颗粒。其中一些策略也已与气体等离子体处理结合应用[89]。但应该考虑到,病毒外壳和基因组的完整性仅代表寄主细胞感染过程中的一部分,因此,活力PCR方法只能近似评估病毒的感染力。
为了预防这些问题并减少对细胞培养进行病毒测试的技术复杂性,通常会提出替代策略,主要是通过使用细菌病毒(噬菌体)来实现。噬菌体的检测和计数采用传统的细菌学技术,并且受测试部分中基质残留物的影响更少。因此,不同的噬菌体已被用作CoV或更普遍地用于包膜病毒的代用品,其中包括Enterobacteria噬菌体MS2(Leviviridae家族)或Pseudomonas phi噬菌体(例如M5方程式或M6方程式,Cystoviridae家族)[80],[86],[87]。然而需要注意的是,噬菌体行为的代表性似乎对气溶胶传播的病毒具有变化性[88],而且这些代用品都不能与CoV完全对应(MS2噬菌体是非包膜病毒,而phi噬菌体具有分段的双链RNA)。规避细胞培养病毒的其他方法包括使用“viability PCR”,即专门设计的分子分析方法,以评估病毒外壳或基因组(或更少见的两者)的完整性。这些方法依赖于特定的分析策略,如使用长模板PCR,涵盖大片段或理想情况下整个病毒基因组来评估其完整性,或使用核酸插入剂,如乙啶单偶氮苯或丙啶单偶氮苯(EMA或PMA),以阻止PCR扩增其中失去外壳完整性导致暴露病毒RNA的病毒颗粒。其中一些策略也已与气体等离子处理结合应用[89]。然而应注意到,病毒外壳和基因组的完整性仅代表寄主细胞感染过程中的一部分,因此, viability PCR方法仅能近似评估病毒的感染能力。
B. 冠状病毒空气净化
在过去几年中,包括 COVID-19 最近的紧急情况期间,一些涉及生物气溶胶传输对于病毒性呼吸道疾病的作用以及空气传播和飞沫传播之间争议的论文是有用的参考。具体来说,Bourouiba 等人[90]考虑了剧烈呼吸事件(咳嗽和打喷嚏)在感染和易感人员密切接触时传输呼吸道疾病的作用。通过交织实验(高速成像技术)和理论研究,该研究引起了人们对悬浮液滴的多相湍流浮力云在潜在地扩大呼吸道病原体范围的重视。敏感的激光散射观察证实,在封闭环境中正常言语可能会导致空气传播的病毒,即使来自 SARS-CoV-2 无症状携带者。同时,大声说话会导致每秒数千个口唾液飞沫的排放[91]。空气传播与飞沫途径的重要性需要得到强调,这与许多呼吸道病毒的传播和随之产生的防空气传播的必要措施在某些情况下密切相关[92]。在这方面,van Doremalen 等人[20]比较了在不同实验条件下(包括空气和物表面上的塑料、不锈钢、纸板和铜基质)SARS-CoV-2 与 SARS-CoV-1 的传播。他们表明病毒在气溶胶中可保持感染能力长达数小时,在表面上可保持数天。这可能解释了医院内部的传播和大规模传播,同时也为控制瘟疫的努力提供了有用的路线图。一种基于等离子体的替代方法是配备带有电池驱动的小型等离子体源的保护口罩,以防止气溶胶致病病毒的传播。
C. 对被冠状病毒污染的体表进行消毒的综合评估
存在直接证据表明,病毒暴露的概率增加了感染的可能性,间接证据表明,初始病毒载量影响感染的严重程度[93],[94]。为了降低病毒载量并在上呼吸道诊断和治疗干预(例如,鼻镜检查、支气管镜检和支气管冲洗)以及牙科治疗之前,在释放有感染性气溶胶之前,使用气体等离子体处理在鼻咽腔中可能是有效的。根据当前的知识状态,SARS-CoV-2的感染性特别严重,因为这种病毒主要在口腔和喉咙区域复制。在感染的早期阶段,COVID-19疾病的症状并不明显或仍然非常缩短,而这些个体的感染性特别高[95]。因此,对于已经进行了阳性测试但尚未感染的个体,早期减少口腔和喉咙区域病毒载量可能会减少其感染性并随后减少甚至消除进一步的病毒传播,同时减少或甚至避免接触限制和隔离的严重经济后果。然而,SARS-CoV-2感染的有效药物治疗尚不可得。或者可以考虑治疗受感染的黏膜组织。为此,还讨论了基于气体等离子体技术的过程。众所周知,空气的等离子体处理对于污染控制非常有用,包括减少空气传播的病原体[96]–[101]。此外,经过等离子体处理的气体或等离子体处理的空气已被证明在材料、表面和货物的微生物净化方面非常有效[102]–[105]。基于这些事实,提出了使用处理过的等离子体空气来减少或消除插管、通气患者口腔和咽喉腔中的病毒载量的想法。同时,也建议使用气体等离子体介导的半胱氨酸氧化可能是改变SARS-CoV-2致病性的一种策略,甚至可以通过手术时的麻醉面罩途径进行注入[106]。然而,虽然这个想法似乎是显而易见的,但一些至关重要的边界条件仍然不能忽视。首先,口腔和喉咙区域的黏膜组织并不是简单的无生命物质,而是敏感的生物组织。因此,为了避免严重的局部损伤和副作用,必须先证明任何黏膜组织的相容性。可能,这可能并不是主要问题,因为最近的一项研究表明,使用kINPen等离子体射流直接对小鼠黏膜组织进行气体等离子体处理是耐受的且没有副作用[107]。更重要的是,在治疗口腔和咽喉区域时对吸入经过处理的等离子体空气的(至少部分)风险进行评估。众所周知,氮(N2)和氧(O2)的等离子体处理空气会产生臭氧(O3)和氮氧化物(NOx)。这两种气体物种一方面对病原体灭活至关重要,但另一方面,如果在更高的浓度下积累,则对肺部有高度毒性。因此,平衡这些气体物种的浓度以实现足够的抗病毒效果并最小化任何副作用可能是一个挑战。因此,要求所有旨在使用经过等离子体处理的呼吸空气来灭活口腔和咽喉区域病毒的方法必须保证并证明任何吸入此空气的毒理学可接受性。
另一个经常讨论的领域是等离子体应用于手部消毒[32],[108],[109]。考虑到SARS-CoV-2的减少,一些等离子体研究所再次启动了这种方法,这并不令人惊讶。正如上面所述,从治疗无生命表面的等离子效果类比到治疗有生命的皮肤必须谨慎解释。除了已经证明皮肤耐受性之外,还必须证明等离子体对手部和皮肤消毒方法的强需求的有效性。
总的来说,还没有提供关于等离子体在像皮肤或黏膜等活体组织中对SARS-CoV-2的特定有效性的证据。
资助声明
Sander Bekeschus和Thomas von Woedtke的工作在一定程度上得到德国教育和研究部(BMBF)的资助,资助编号为03Z22DN11,03Z22DN12和03Z22Di1,以及欧洲社会基金会的资助,资助编号为ESF/14-BM-A55-0006-18。Elisabetta Suffredini的工作得到MIUR PRIN 2017项目PlasmaFood的资助。Vittorio Colombo的工作在一定程度上得到2014—2020年欧洲区域发展基金Emilia-Romagna区域运营计划关于工业研究和创新项目对抗COVID-19传播解决方案的资助,项目名称为VIrus KIller (VIKI),以及MIUR PRIN 2017项目PlasmaFood的资助。
引用:
[1] Bar-On Y. M., Flamholz A., Phillips R., and Milo R., “SARS-CoV-2 (COVID-19) by the numbers,” Elife, vol. 9, Apr. 2020, Art. no. e57309. [PMC free article] [PubMed] [Google Scholar]
[2] Stadler K.et al., “SARS—Beginning to understand a new virus,” Nat. Rev. Microbiol., vol. 1, no. 3, pp. 209–218, Dec. 2003. [PMC free article] [PubMed] [Google Scholar]
[3] Zhao Z.et al., “Moderate mutation rate in the SARS coronavirus genome and its implications,” BMC Evol. Biol., vol. 4, no. p. 21, Jun. 2004. [PMC free article] [PubMed] [Google Scholar]
[4] Robertson D. L., Singer J. B., Orton R. J., and MacLean O. A., “No evidence for distinct types in the evolution of SARS-CoV-2,” Virus Evol., vol. 6, no. 1, 2020, Art. no. veaa034. [PMC free article] [PubMed] [Google Scholar]
[5] Forster P., Forster L., Renfrew C., and Forster M., “Phylogenetic network analysis of SARS-CoV-2 genomes,” Proc. Nat. Acad. Sci. USA, vol. 117, no. 17, pp. 9241–9243, Apr. 2020. [PMC free article] [PubMed] [Google Scholar]
[6] Eterpi M., McDonnell G., and Thomas V., “Disinfection efficacy against parvoviruses compared with reference viruses,” J. Hospital Infection, vol. 73, no. 1, pp. 64–70, Sep. 2009. [PubMed] [Google Scholar]
[7] Howie R., Alfa M. J., and Coombs K., “Survival of enveloped and non-enveloped viruses on surfaces compared with other micro-organisms and impact of suboptimal disinfectant exposure,” J. Hospital Infection, vol. 69, no. 4, pp. 368–376, Aug. 2008. [PubMed] [Google Scholar]
[8] International Committee on Taxonomy of Viruses Executive, “The new scope of virus taxonomy: Partitioning the virosphere into 15 hierarchical ranks,” Nat. Microbiol., vol. 5, no. 5, pp. 668–674, May 2020. [PMC free article] [PubMed] [Google Scholar]
[9] Braithwaite N. S. J., “Introduction to gas discharges,” Plasma Sources Sci. Technol., vol. 9, no. 4, pp. 517–527, Nov. 2000. [Google Scholar]
[10] Conrads H. and Schmidt M., “Plasma generation and plasma sources,” Plasma Sources Sci. Technol., vol. 9, no. 4, pp. 441–454, Nov. 2000. [Google Scholar]
[11] Bogaerts A., Neyts E., Gijbels R., and van der Mullen J., “Gas discharge plasmas and their applications,” Spectrochimica Acta B Atomic Spectroscopy, vol. 57, no. 4, pp. 609–658, Apr. 2002. [Google Scholar]
[12] von Woedtke T., Metelmann H. R., and Weltmann K. D., “Clinical plasma medicine: State and perspectives of in vivo application of cold atmospheric plasma,” Contrib. Plasma Phys., vol. 54, no. 2, pp. 104–117, 2014. [Google Scholar]
[13] Isbary G.et al., “Cold atmospheric plasma devices for medical issues,” Expert Rev. Med. Devices, vol. 10, no. 3, pp. 367–377, May 2013. [PubMed] [Google Scholar]
[14] Lu X., Laroussi M., and Puech V., “On atmospheric-pressure non-equilibrium plasma jets and plasma bullets,” Plasma Sources Sci. Technol., vol. 21, no. 3, Jun. 2012, Art. no. 034005. [Google Scholar]
[15] Zou L.et al., “SARS-CoV-2 viral load in upper respiratory specimens of infected patients,” New England J. Med., vol. 382, no. 12, pp. 1177–1179, Mar. 2020. [PMC free article] [PubMed] [Google Scholar]
[16] Judson S. D. and Munster V. J., “Nosocomial transmission of emerging viruses via aerosol-generating medical procedures,” Viruses, vol. 11, no. 10, p. 940, Oct. 2019. [PMC free article] [PubMed] [Google Scholar]
[17] Wang W.et al., “Detection of SARS-CoV-2 in different types of clinical specimens,” J. Amer. Med. Assoc., vol. 323, no. 18, pp. 1843–1844, Mar. 2020. [PMC free article] [PubMed] [Google Scholar]
[18] Young B. E.et al., “Epidemiologic features and clinical course of patients infected with SARS-CoV-2 in Singapore,” J. Amer. Med. Assoc., vol. 323, no. 15, pp. 1488–1494, Mar. 2020. [PMC free article] [PubMed] [Google Scholar]
[19] Rafiq D., Batool A., and Bazaz M. A., “Three months of COVID-19: A systematic review and meta-analysis,” Rev. Med. Virol., to be published. [Online]. Available: https://onlinelibrary.wiley.com/doi/full/10.1002/rmv.2113
[20] van Doremalen N.et al., “Aerosol and surface stability of SARS-CoV-2 as compared with SARS-CoV-1,” New England J. Med., vol. 382, no. 16, pp. 1564–1567, Apr. 2020. [PMC free article] [PubMed] [Google Scholar]
[21] Rabenau H. F., Cinatl J., Morgenstern B., Bauer G., Preiser W., and Doerr H. W., “Stability and inactivation of SARS coronavirus,” Med. Microbiol. Immunol., vol. 194, nos. 1–2, pp. 1–6, Jan. 2005. [PMC free article] [PubMed] [Google Scholar]
[22] Weiss M.et al., “Virucide properties of cold atmospheric plasma for future clinical applications,” J. Med. Virol., vol. 89, no. 6, pp. 952–959, Jun. 2017. [PubMed] [Google Scholar]
[23] Kramer A., Schauer F., Papke R., and Bekeschus S., “Plasma application for hygienic purposes in medicine, industry, and biotechnology: Update 2017,” in Comprehensive Clinical Plasma Medicine, Metelmann H.-R., von Woedtke T., and Weltmann K.-D., Eds. Cham, Switzerland: Springer Int., 2018, pp. 253–281. [Google Scholar]
[24] Wang G.et al., “Non-thermal plasma for inactivated-vaccine preparation,” Vaccine, vol. 34, no. 8, pp. 1126–1132, Feb. 2016. [PubMed] [Google Scholar]
[25] Sakudo A., Toyokawa Y., Imanishi Y., and Murakami T., “Crucial roles of reactive chemical species in modification of respiratory syncytial virus by nitrogen gas plasma,” Mater. Sci. Eng. C Mater. Biol. Appl., vol. 74, pp. 131–136, May 2017. [PubMed] [Google Scholar]
[26] Romero-Mangado J.et al., “Efficacy of atmospheric pressure dielectric barrier discharge for inactivating airborne pathogens,” J. Vacuum Sci. Technol. A Vacuum Surfaces Films, vol. 35, no. 4, 2017, Art. no. 041101. [Google Scholar]
[27] Romero-Mangado J.et al., “Morphological and chemical changes of aerosolized E. Coli treated with a dielectric barrier discharge,” Biointerphases, vol. 11, no. 2, Mar. 2016, Art. no. 011009. [PubMed] [Google Scholar]
[28] Wu Y.et al., “MS2 virus inactivation by atmospheric-pressure cold plasma using different gas carriers and power levels,” Appl. Environ. Microbiol., vol. 81, no. 3, pp. 996–1002, 2015. [PMC free article] [PubMed] [Google Scholar]
[29] Xia T., Kleinheksel A., Lee E. M., Qiao Z., Wigginton K. R., and Clack H. L., “Inactivation of airborne viruses using a packed bed non-thermal plasma reactor,” J. Phys. D Appl. Phys., vol. 52, no. 25, Jun. 2019, Art. no. 255201. [PMC free article] [PubMed] [Google Scholar]
[30] von Woedtke T., Kramer A., and Weltmann K.-D., “Plasma sterilization: What are the conditions to meet this claim?” Plasma Process. Polym., vol. 5, no. 6, pp. 534–539, 2008. [Google Scholar]
[31] Bekeschus S., Favia P., Robert E., and von Woedtke T., “White paper on plasma for medicine and hygiene: Future in plasma health sciences,” Plasma Process. Polym., vol. 16, no. 1, Jan. 2019, Art. no. 1800033. [Google Scholar]
[32] Kramer A.et al., “Cold physical plasmas in the field of hygiene-relevance, significance, and future applications,” Plasma Process. Polym., vol. 12, no. 12, pp. 1410–1422, Dec. 2015. [Google Scholar]
[33] Fiebrandt M., Lackmann J.-W., and Stapelmann K., “From patent to product? 50 years of low-pressure plasma sterilization,” Plasma Process. Polym., vol. 15, no. 12, 2018, Art. no. 1800139. [Google Scholar]
[34] Scholtz V., Pazlarova J., Souskova H., Khun J., and Julak J., “Nonthermal plasma—A tool for decontamination and disinfection,” Biotechnol. Adv., vol. 33, no. 6, pp. 1108–1119, Nov. 2015. [PubMed] [Google Scholar]
[35] OConnor N., Cahill O., Daniels S., Galvin S., and Humphreys H., “Cold atmospheric pressure plasma and decontamination. Can it contribute to preventing hospital-acquired infections?” J. Hospital Infection, vol. 88, no. 2, pp. 59–65, Oct. 2014. [PubMed] [Google Scholar]
[36] Moreau M., Orange N., and Feuilloley M. G., “Non-thermal plasma technologies: New tools for bio-decontamination,” Biotechnol. Adv., vol. 26, no. 6, pp. 610–617, Nov-Dec 2008. [PubMed] [Google Scholar]
[37] Mai-Prochnow A., Murphy A. B., McLean K. M., Kong M. G., and Ostrikov K. K., “Atmospheric pressure plasmas: Infection control and bacterial responses,” Int. J. Antimicrobial Agents, vol. 43, no. 6, pp. 508–517, Jun. 2014. [PubMed] [Google Scholar]
[38] Pârvulescu V. I., Magureanu M., and Lukes P., Plasma Chemistry and Catalysis in Gases and Liquids. Hoboken, NJ, USA: Wiley, 2012. [Google Scholar]
[39] Bathina M. N., Mickelsen S., Brooks C., Jaramillo J., Hepton T., and Kusumoto F. M., “Safety and efficacy of hydrogen peroxide plasma sterilization for repeated use of electrophysiology catheters,” J. Amer. College Cardiol., vol. 32, no. 5, pp. 1384–1388, 1998. [PubMed] [Google Scholar]
[40] Okpara-Hofmann J., Knoll M., Durr M., Schmitt B., and Borneff-Lipp M., “Comparison of low-temperature hydrogen peroxide gas plasma sterilization for endoscopes using various Sterrad models,” J. Hospital Infection, vol. 59, no. 4, pp. 280–285, Apr. 2005. [PubMed] [Google Scholar]
[41] Sakudo A., Yagyu Y., and Onodera T., “Disinfection and sterilization using plasma technology: Fundamentals and future perspectives for biological applications,” Int. J. Mol. Sci., vol. 20, no. 20, p. 5216, Oct. 2019. [PMC free article] [PubMed] [Google Scholar]
[42] Misra N., Schlüter O., and Cullen P. J., Cold Plasma in Food and Agriculture: Fundamentals and Applications. Amsterdam, The Netherlands: Academic, 2016. [Google Scholar]
[43] Magureanu M., Mandache N. B., and Parvulescu V. I., “Degradation of pharmaceutical compounds in water by non-thermal plasma treatment,” Water Res., vol. 81, pp. 124–136, Sep. 2015. [PubMed] [Google Scholar]
[44] Lademann J.et al., “Risk assessment of the application of a plasma jet in dermatology,” J. Biomed. Opt., vol. 14, no. 5, Sep-Oct 2009, Art. no. 054025. [PubMed] [Google Scholar]
[45] Lademann J.et al., “Antisepsis of the skin by treatment with tissue-tolerable plasma (TTP): Risk assessment and perspectives,” in Plasma for Bio-Decontamination, Medicine and Food Security. Dordrecht, The Netherlands: Springer, 2012, pp. 281–291. [Google Scholar]
[46] Lademann J.et al., “Comparison of the antiseptic efficacy of tissue-tolerable plasma and an octenidine hydrochloride-based wound antiseptic on human skin,” Skin Pharmacol. Physiol., vol. 25, no. 2, pp. 100–106, 2012. [PubMed] [Google Scholar]
[47] Klebes M.et al., “Combined antibacterial effects of tissue-tolerable plasma and a modern conventional liquid antiseptic on chronic wound treatment,” J. Biophoton., vol. 8, no. 5, pp. 382–391, May 2015. [PubMed] [Google Scholar]
[48] Daeschlein G.et al., “Skin decontamination by low-temperature atmospheric pressure plasma jet and dielectric barrier discharge plasma,” J. Hospital Infection, vol. 81, no. 3, pp. 177–183, Jul. 2012. [PubMed] [Google Scholar]
[49] Daeschlein G.et al., “Cold plasma is well-tolerated and does not disturb skin barrier or reduce skin moisture,” J. der Deutschen Dermatologischen Gesellschaft, vol. 10, no. 7, pp. 509–515, Jul. 2012. [PubMed] [Google Scholar]
[50] Terrier O.et al., “Cold oxygen plasma technology efficiency against different airborne respiratory viruses,” J. Clin. Virol., vol. 45, no. 2, pp. 119–124, Jun. 2009. [PubMed] [Google Scholar]
[51] Zimmermann J. L.et al., “Effects of cold atmospheric plasmas on adenoviruses in solution,” J. Phys. D Appl. Phys., vol. 44, no. 50, 2011, Art. no. 505201. [Google Scholar]
[52] Brun P.et al., “Disinfection of ocular cells and tissues by atmospheric-pressure cold plasma,” PLoS ONE, vol. 7, no. 3, 2012, Art. no. e33245. [PMC free article] [PubMed] [Google Scholar]
[53] Alekseev O., Donovan K., Limonnik V., and Azizkhan-Clifford J., “Nonthermal dielectric barrier discharge (DBD) plasma suppresses herpes simplex virus type 1 (HSV-1) replication in corneal epithelium,” Transl. Vis. Sci. Technol., vol. 3, no. 2, p. 2, Mar. 2014. [PMC free article] [PubMed] [Google Scholar]
[54] Shi X. M.et al., “Destructive effect of DBCD plasma on HBsAg in human blood and its impact on erythrocyte functions,” IEEE Trans. Plasma Sci., vol. 44, no. 9, pp. 1815–1822, Sep. 2016. [Google Scholar]
[55] Volotskova O., Dubrovsky L., Keidar M., and Bukrinsky M., “Cold atmospheric plasma inhibits HIV-1 replication in macrophages by targeting both the virus and the cells,” PLoS ONE, vol. 11, no. 10, Oct. 2016, Art. no. e0165322. [PMC free article] [PubMed] [Google Scholar]
[56] Amiran M. R., Sepahi A. A., Zabiollahi R., Ghomi H., Momen S. B., and Aghasadeghi M. R., “In vitro assessment of antiviral activity of cold atmospheric pressure plasma jet against the human immunodeficiency virus (HIV),” J. Med. Microbiol. Infectious Diseases, vol. 4, no. 3, pp. 62–67, 2016. [Google Scholar]
[57] Sakudo A., Shimizu N., Imanishi Y., and Ikuta K., “N2 gas plasma inactivates influenza virus by inducing changes in viral surface morphology, protein, and genomic RNA,” Biomed Res. Int., vol. 2013, Sep. 2013, Art. no. 694269. [PMC free article] [PubMed] [Google Scholar]
[58] Guo L.et al., “Mechanism of virus inactivation by cold atmospheric-pressure plasma and plasma-activated water,” Appl. Environ. Microbiol., vol. 84, no. 17, Sep. 2018, Art. no. e00726. [PMC free article] [PubMed] [Google Scholar]
[59] Filipic A., Gutierrez-Aguirre I., Primc G., Mozetic M., and Dobnik D., “Cold plasma, a new hope in the field of virus inactivation,” Trends Biotechnol., to be published. [PMC free article] [PubMed]
[60] Aboubakr H. A., Gangal U., Youssef M. M., Goyal S. M., and Bruggeman P. J., “Inactivation of virus in solution by cold atmospheric pressure plasma: Identification of chemical inactivation pathways,” J. Phys. D Appl. Phys., vol. 49, no. 20, 2016, Art. no. 204001. [Google Scholar]
[61] Kluge S.et al., “Investigating the mutagenicity of a cold argon-plasma jet in an HET-MN model,” PLoS ONE, vol. 11, no. 9, 2016, Art. no. e0160667. [PMC free article] [PubMed] [Google Scholar]
[62] Bekeschus S.et al., “High throughput image cytometry micronucleus assay to investigate the presence or absence of mutagenic effects of cold physical plasma,” Environ. Mol. Mutagen., vol. 59, no. 4, pp. 268–277, May 2018. [PubMed] [Google Scholar]
[63] Wende K.et al., “Risk assessment of a cold argon plasma jet in respect to its mutagenicity,” Mutation Res. Genet. Toxicol. Environ. Mutagenesis, vols. 798–799, pp. 48–54, Mar. 2016. [PubMed] [Google Scholar]
[64] Bekeschus S.et al., “Elevated H2AX phosphorylation observed with kINPen plasma treatment is not caused by ROS-mediated DNA damage but is the consequence of apoptosis,” Oxidative Med. Cellular Longevity, vol. 2019, Sep. 2019, Art. no. 8535163. [PMC free article] [PubMed] [Google Scholar]
[65] Privat-Maldonado A.et al., “ROS from physical plasmas: Redox chemistry for biomedical therapy,” Oxidative Med. Cellular Longevity, vol. 2019, Oct. 2019, Art. no. 9062098. [PMC free article] [PubMed] [Google Scholar]
[66] Hasse S.et al., “Cold argon plasma as adjuvant Tumour therapy on progressive head and neck cancer: A preclinical study,” Appl. Sci., vol. 9, no. 10, p. 2061, May 2019. [Google Scholar]
[67] Rödder K.et al., “Activation of murine immune cells upon co-culture with plasma-treated B16F10 melanoma cells,” Appl. Sci., vol. 9, no. 4, p. 660, 2019. [Google Scholar]
[68] Bekeschus S., Seebauer C., Wende K., and Schmidt A., “Physical plasma and leukocytes—Immune or reactive?” Biol. Chem., vol. 400, no. 1, pp. 63–75, Dec. 2018. [PubMed] [Google Scholar]
[69] Bekeschus S.et al., “Plasma treatment of ovarian cancer cells mitigates their immuno-modulatory products active on THP-1 monocytes,” Plasma, vol. 1, no. 1, pp. 201–217, 2018. [Google Scholar]
[70] Gorse G. J., OConnor T. Z., Hall S. L., Vitale J. N., and Nichol K. L., “Human coronavirus and acute respiratory illness in older adults with chronic obstructive pulmonary disease,” J. Infect. Disord., vol. 199, no. 6, pp. 847–857, Mar. 2009. [PMC free article] [PubMed] [Google Scholar]
[71] Pyrc K.et al., “Culturing the unculturable: Human coronavirus HKU1 infects, replicates, and produces progeny virions in human ciliated airway epithelial cell cultures,” J. Virol., vol. 84, no. 21, pp. 11255–11263, Nov. 2010. [PMC free article] [PubMed] [Google Scholar]
[72] Blanco A.et al., “Glass wool concentration optimization for the detection of enveloped and non-enveloped waterborne viruses,” Food Environ. Virol., vol. 11, no. 2, pp. 184–192, Jun. 2019. [PMC free article] [PubMed] [Google Scholar]
[73] Farnsworth J. E.et al., “Development of a method for bacteria and virus recovery from heating, ventilation, and air conditioning (HVAC) filters,” J. Environ. Monitor., vol. 8, no. 10, pp. 1006–1013, Oct. 2006. [PubMed] [Google Scholar]
[74] Goyal S. M., Chander Y., Yezli S., and Otter J. A., “Evaluating the virucidal efficacy of hydrogen peroxide vapour,” J. Hospital Infection, vol. 86, no. 4, pp. 255–259, Apr. 2014. [PMC free article] [PubMed] [Google Scholar]
[75] Hulkower R. L., Casanova L. M., Rutala W. A., Weber D. J., and Sobsey M. D., “Inactivation of surrogate coronaviruses on hard surfaces by health care germicides,” Amer. J. Infect. Control, vol. 39, no. 5, pp. 401–407, Jun. 2011. [PMC free article] [PubMed] [Google Scholar]
[76] Casanova L. M., Jeon S., Rutala W. A., Weber D. J., and Sobsey M. D., “Effects of air temperature and relative humidity on coronavirus survival on surfaces,” Appl. Environ. Microbiol., vol. 76, no. 9, pp. 2712–2717, May 2010. [PMC free article] [PubMed] [Google Scholar]
[77] Casanova L., Rutala W. A., Weber D. J., and Sobsey M. D., “Survival of surrogate coronaviruses in water,” Water Res., vol. 43, no. 7, pp. 1893–1898, Apr. 2009. [PMC free article] [PubMed] [Google Scholar]
[78] Gundy P. M., Gerba C. P., and Pepper I. L., “Survival of coronaviruses in water and wastewater,” Food Environ. Virol., vol. 1, no. 1, p. 10, 2008. [Google Scholar]
[79] Dellanno C., Vega Q., and Boesenberg D., “The antiviral action of common household disinfectants and antiseptics against murine hepatitis virus, a potential surrogate for SARS coronavirus,” Amer. J. Infect. Control, vol. 37, no. 8, pp. 649–652, Oct. 2009. [PMC free article] [PubMed] [Google Scholar]
[80] Ye Y., Ellenberg R. M., Graham K. E., and Wigginton K. R., “Survivability, partitioning, and recovery of enveloped viruses in untreated municipal wastewater,” Environ. Sci. Technol., vol. 50, no. 10, pp. 5077–5085, May 2016. [PMC free article] [PubMed] [Google Scholar]
[81] Abd-Elmaksoud S., Spencer S. K., Gerba C. P., Tamimi A. H., Jokela W. E., and Borchardt M. A., “Simultaneous concentration of bovine viruses and agricultural zoonotic bacteria from water using sodocalcic glass wool filters,” Food Environ. Virol., vol. 6, no. 4, pp. 253–259, Dec. 2014. [PMC free article] [PubMed] [Google Scholar]
[82] Millet J. K.et al., “Production of pseudotyped particles to study highly pathogenic coronaviruses in a biosafety level 2 setting,” J. Vis. Exp., vol. 145, Mar. 2019, Art. no. e59010. [PMC free article] [PubMed] [Google Scholar]
[83] Pu T.et al., “Evaluate severe acute respiratory syndrome coronavirus 2 infectivity by pseudoviral particles,” J. Med. Virol., to be published. [PMC free article] [PubMed]
[84] Richards G. P., “Critical review of norovirus surrogates in food safety research: Rationale for considering volunteer studies,” Food Environ. Virol., vol. 4, no. 1, pp. 6–13, Mar. 2012. [PMC free article] [PubMed] [Google Scholar]
[85] La Rosa G., Bonadonna L., Lucentini L., Kenmoe S., and Suffredini E., “Coronavirus in water environments: Occurrence, persistence and concentration methods—A scoping review,” Water Res., vol. 179, Jul. 2020, Art. no. 115899. [PMC free article] [PubMed] [Google Scholar]
[86] Gendron L., Verreault D., Veillette M., Moineau S., and Duchaine C., “Evaluation of filters for the sampling and quantification of RNA phage aerosols,” Aerosol Sci. Technol., vol. 44, no. 10, pp. 893–901, 2010. [Google Scholar]
[87] Aquino de Carvalho N., Stachler E. N., Cimabue N., and Bibby K., “Evaluation of Phi6 persistence and suitability as an enveloped virus surrogate,” Environ. Sci. Technol., vol. 51, no. 15, pp. 8692–8700, Aug. 2017. [PubMed] [Google Scholar]
[88] Turgeon N., Toulouse M. J., Martel B., Moineau S., and Duchaine C., “Comparison of five bacteriophages as models for viral aerosol studies,” Appl. Environ. Microbiol., vol. 80, no. 14, pp. 4242–4250, Jul. 2014. [PMC free article] [PubMed] [Google Scholar]
[89] Aboubakr H. A., Sampedro Parra F., Collins J., Bruggeman P., and Goyal S. M., “In situ inactivation of human norovirus GII.4 by cold plasma: Ethidium monoazide (EMA)-coupled RT-qPCR underestimates virus reduction and fecal material suppresses inactivation,” Food Microbiol., vol. 85, Feb. 2020, Art. no. 103307. [PubMed] [Google Scholar]
[90] Bourouiba L., Dehandschoewercker E., and Bush J. W. M., “Violent expiratory events: On coughing and sneezing,” J. Fluid Mech., vol. 745, pp. 537–563, Apr. 2014. [Google Scholar]
[91] Stadnytskyi V., Bax C. E., Bax A., and Anfinrud P., “The airborne lifetime of small speech droplets and their potential importance in SARS-CoV-2 transmission,” Proc. Nat. Acad. Sci. USA, vol. 117, no. 22, pp. 11875–11877, Jun. 2020. [PMC free article] [PubMed] [Google Scholar]
[92] Shiu E. Y. C., Leung N. H. L., and Cowling B. J., “Controversy around airborne versus droplet transmission of respiratory viruses,” Current Opin. Infectious Diseases, vol. 32, no. 4, pp. 372–379, 2019. [PubMed] [Google Scholar]
[93] Heinzerling A.et al., “Transmission of COVID-19 to health care personnel during exposures to a hospitalized patient—Solano County, California, February 2020,” Morbidity Mortality Weekly Rep., vol. 69, no. 15, pp. 472–476, Apr. 2020. [PMC free article] [PubMed] [Google Scholar]
[94] Raoult D., Zumla A., Locatelli F., Ippolito G., and Kroemer G., “Coronavirus infections: Epidemiological, clinical and immunological features and hypotheses,” Cell Stress, vol. 4, no. 4, pp. 66–75, Mar. 2020. [PMC free article] [PubMed] [Google Scholar]
[95] Wolfel R.et al., “Virological assessment of hospitalized patients with COVID-2019,” Nature, vol. 581, no. 7809, pp. 465–469, May 2020. [PubMed] [Google Scholar]
[96] Muller S. and Zahn R. J., “Air pollution control by non-thermal plasma,” Contrib. Plasma Phys., vol. 47, no. 7, pp. 520–529, 2007. [Google Scholar]
[97] Ondarts M., Hajji W., Outin J., Bejat T., and Gonze E., “Non-thermal plasma for indoor air treatment: Toluene degradation in a corona discharge at PPBV levels,” Chem. Eng. Res. Des., vol. 118, pp. 194–205, Feb. 2017. [Google Scholar]
[98] Brandenburg R.et al., “Plasma-based pollutant degradation in gas streams: Status, examples and outlook,” Contrib. Plasma Phys., vol. 54, no. 2, pp. 202–214, Feb. 2014. [Google Scholar]
[99] Lai A. C. K., Cheung A. C. T., Wong M. M. L., and Li W. S., “Evaluation of cold plasma inactivation efficacy against different airborne bacteria in ventilation duct flow,” Build. Environ., vol. 98, pp. 39–46, Mar. 2016. [Google Scholar]
[100] Ki S. H., Masur K., Baik K. Y., and Choi E. H., “Effects of humidity on room disinfection by dielectric barrier discharge plasma,” J. Phys. D Appl. Phys., vol. 52, no. 42, 2019, Art. no. 425204. [Google Scholar]
[101] Karatum O. and Deshusses M. A., “A comparative study of dilute VOCs treatment in a non-thermal plasma reactor,” Chem. Eng. J., vol. 294, pp. 308–315, Jun. 2016. [Google Scholar]
[102] Bhatt S.et al., “Efficacy of low-temperature plasma-activated gas disinfection against biofilm on contaminated GI endoscope channels,” Gastrointestinal Endoscopy, vol. 89, no. 1, pp. 105–114, Jan. 2019. [PubMed] [Google Scholar]
[103] Ehlbeck J.et al., “Plasma treatment of food,” Contrib. Plasma Phys., vol. 55, no. 10, pp. 753–757, 2015. [Google Scholar]
[104] Schnabel U.et al., “Decontamination of microbiologically contaminated seeds by microwave driven discharge processed gas,” J. Agricult. Sci. Appl., vol. 1, no. 4, pp. 100–106, 2012. [Google Scholar]
[105] Schnabel U., Schmidt C., Stachowiak J., Bösel A., Andrasch M., and Ehlbeck J., “Plasma processed air for biological decontamination of PET and fresh plant tissue,” Plasma Process. Polym., vol. 15, no. 2, 2018, Art. no. 1600057. [Google Scholar]
[106] Ghanavi J., Farnia P., and Ghomi H., “The effectiveness of cold atmospheric plasma by inhaling anesthetic mask or through bronchoscopy against COVID-19,” Biomed. Biotechnol. Res. J., vol. 4, no. 1, p. 1, 2020. [Google Scholar]
[107] Jablonowski L.et al., “Side effects by oral application of atmospheric pressure plasma on the mucosa in mice,” PLoS ONE, vol. 14, no. 4, 2019, Art. no. e0215099. [PMC free article] [PubMed] [Google Scholar]
[108] Kong M. G.et al., “Plasma medicine: An introductory review,” New J. Phys., vol. 11, no. 11, Nov. 2009, Art. no. 115012. [Google Scholar]
[109] Boyce J. M., “Update on hand hygiene,” Amer. J. Infect. Control, vol. 41, no. 5, pp. 94–96, May 2013. [Google Scholar]